
Nearly 6 million Americans have opioid use disorder (OUD), but only 1 in 5 receive treatment.1,2
This module helps primary care clinicians identify and diagnose patients with opioid use disorder, understand the role of medication for OUD, learn a process to initiate buprenorphine in patients with OUD, and learn about harm reduction strategies, including recommending or prescribing naloxone.
Defining opioid use disorder
OUD is problematic opioid use that leads to clinically significant impairment or distress. It is marked by at least two of the following over the past 12 months.3
- using opioids at higher doses or longer than intended
- unsuccessful attempts to control or reduce use
- significant time lost obtaining, consuming, or recovering from opioids
- cravings for opioids
- failure to fulfill obligations because of opioids
- persistent social or interpersonal problems caused by opioids
- opioid use displaces social, work, or recreational activities
- using opioids in hazardous situations (e.g., while driving)
- use continues despite physical or psychological problems caused or worsened by opioids
- tolerance: a reduced effect of the drug despite increasing dosages (in patients taking opioids other than as prescribed)
- withdrawal (in patients taking opioids other than as prescribed
OUD results from a combination of factors such as environment, biology or genetics, and the drug used.4
Opioid dependence does not equal opioid addiction5
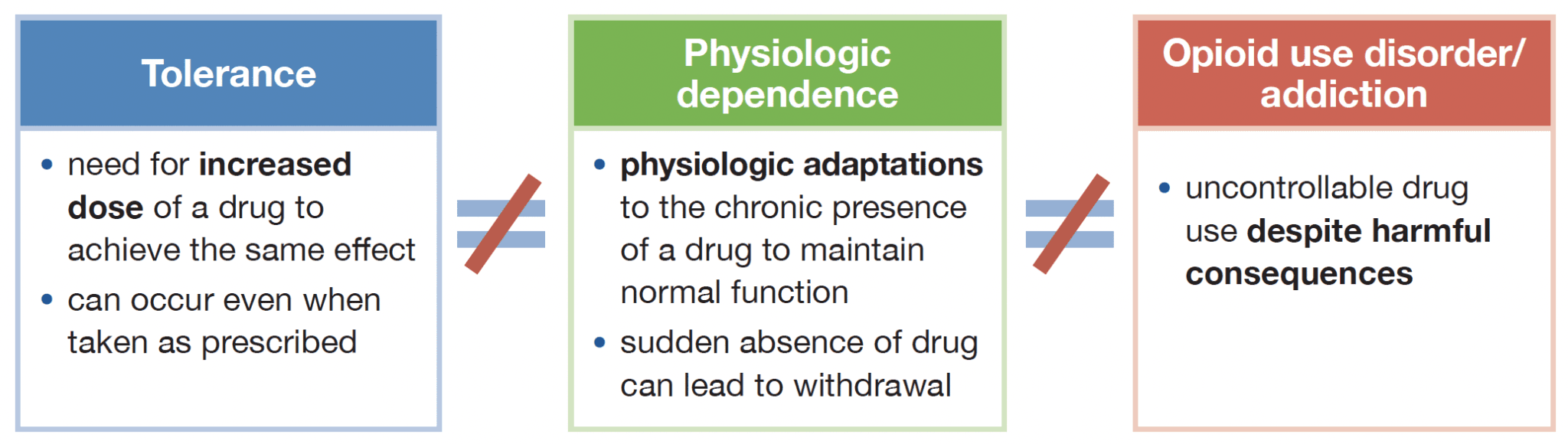
Patients who take opioids as prescribed without impairment of daily life do NOT have an addiction.
Primary care providers play an integral role in identifying patients with OUD. Adding questions about opioid misuse to annual screening questions about tobacco and alcohol create an opportunity to discuss or uncover problematic behaviors. Screening, Brief Intervention, and Referral to Treatment (SBIRT) provides a framework for assessing patients reporting problematic behaviors, engaging patients in behavior change, and linking them into any needed treatment.5
Medications to treat OUD
Three medications are FDA-approved to treat OUD: buprenorphine, methadone, and naltrexone extended-release injection. All of these options can improve retention in treatment, increase time without opioid misuse, and reduce mortality.
Buprenorphine is one of the most effective interventions available. For every 5 people treated with buprenorphine for OUD, 1 life will be saved.6 Buprenorphine can safely be initiated at home in many patients. New dosing protocols allow for new ways to initiate buprenorphine at home or in the emergency department.
Clinicians can treat OUD with medication even without access to concurrent behavioral treatment.7,8
Harm reduction
Implement strategies to reduce the risk of overdose or morbidity from OUD.
- Prescribe or discuss naloxone.
- Recommend routine immunization, especially for hepatitis, pneumococcus, and tetanus.
- Screen for infections, especially HIV and hepatitis C.
- For patients who typically use alone, recommend www.neverusealone.com or the 1-800-484-3731 hotline to prevent unintentional overdose.
- Discuss sterile injection practices to reduce transmission of blood-borne pathogens like HIV and hepatitis C, link with a syringe exchange program (if available), or prescribe insulin needles.
- Recommend fentanyl test strips, if available.
- Evaluate whether pre-exposure prophylaxis (PrEP) is indicated for HIV prevention.
Resources for Providers
- Prescribing Naloxone
- What is SBIRT?
- SBIRT Billing
- Tobacco, Alcohol, Prescription medication, and other Substance use (TAPS) Tool
- Drug Abuse Screening Tool (DAST-10)
- Providers’ Clinical Support System
- Clinical opiate withdrawal scale (COWS)
Buprenorphine Dosing Strategies
- Low dose or Microdosing protocol from Bridge to Treatment
- Classic dosing protocol from BMC Grayken Center
- High dose or Macrodosing protocol from Bridge to Treatment
State Specific Resources
- Delaware – Addiction treatment and recovery resources
- New Hampshire – Substance use prevention, misuse, and treatment resources
- Pennsylvania – Opioid dashboard
Click here to contact us for more information about Alosa’s full academic detailing package.